If you’re evaluating whether to open or invest in a medical clinic, one of the first questions you should be asking is this: how does a medical clinic business actually generate revenue?
The answer is more layered than most people expect. A clinic isn’t just billing for doctor’s visits. The most profitable clinics operate with multiple, stacked revenue streams — some predictable and recurring, others high-margin and cash-based. Understanding each of these revenue drivers is what separates a clinic that barely breaks even from one that builds real wealth.
This article breaks it all down service by service, stream by stream so you can make an informed decision before committing capital or time.
Understand: Cost to start Medical Care Clinic Business
The Revenue Model of a Medical Clinic: How It Actually Works
At its core, a medical clinic generates revenue by providing healthcare services and getting paid for them by patients directly, by insurance companies, or by government programs like Medicare and Medicaid.
But the structure of how and from whom you collect that revenue determines your cash flow stability, your margins, and how quickly you can scale.
Fee-for-service models remain the dominant revenue structure for most clinics, but successful medical clinics increasingly diversify their income through chronic care management programs, Medicare Shared Savings Programs, and value-based care bonuses.
Here’s a complete look at every revenue driver your clinic can tap.
Revenue Driver #1 — Patient Consultations (The Foundation)
Patient consultations are the bedrock of any clinic’s income. A patient books an appointment, sees a provider, and the clinic bills for that encounter.
General consultations form the foundation of clinic revenue, generating $100 to $200 per patient visit. These routine appointments provide steady, predictable income but operate at lower profit margins due to the high volume of time investment required per patient.
The revenue per consultation varies based on:
- Specialty: A primary care visit averages $100–$200, while a specialist consultation can range from $150 to $500+
- Visit complexity: Higher CPT billing codes mean more revenue per encounter
- Payer mix: Commercial insurance patients generally reimburse at higher rates than Medicaid
One critical metric here is your net collection rate — what you actually collect versus what you bill. Medical clinics typically collect between 60% and 75% of their original billed charges after accounting for insurance adjustments, contractual write-offs, and patient non-payment. A clinic billing $1,000 per day per provider with a 65% collection rate actually receives only $650 in real revenue.
This gap between gross charges and actual collections is where many clinic owners are surprised. Your revenue model must account for it from Day 1.
Revenue Driver #2 — Diagnostic and Ancillary Services (High-Margin Add-ons)
Diagnostic services i.e. lab tests, X-rays, ultrasounds, EKGs are one of the most lucrative secondary revenue sources a clinic can develop. You’re already seeing the patient. Running a lab panel or imaging study during the same visit adds revenue with minimal additional overhead.
Medical clinics derive revenue from different sources, including patient consultations, diagnostic tests, procedures, and ancillary services. Tests such as blood work, X-rays, or ultrasounds generate additional revenue for the clinic, with charges varying depending on the complexity and equipment required.
Ancillary revenue streams include:
- In-house laboratory (CBC, lipid panels, HbA1c, urinalysis)
- On-site imaging (X-ray, ultrasound)
- Physical therapy and rehabilitation services
- Nutrition counseling and dietitian services
- Mental health services integrated into primary care
These services are powerful revenue drivers because they leverage the same patient relationship. A single primary care visit can become a $300–$500 encounter when ancillary services are bundled in.
Revenue Driver #3 — Specialty and Procedure-Based Services (Your Highest-Margin Revenue)
This is where the real financial upside lives. Specialty procedures command significantly higher reimbursements per encounter and many of them are cash-pay, which means you get paid immediately without waiting for insurance processing.
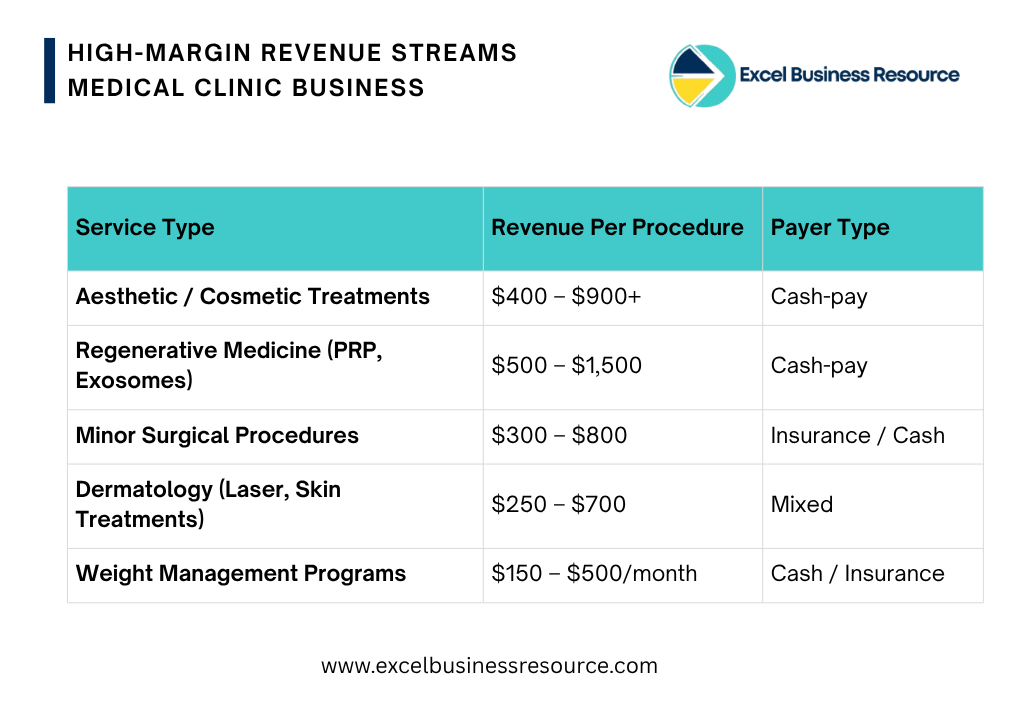
Specialty services represent the most profitable segment for modern clinics. Regenerative therapy, aesthetic treatments, and medspa services command $400 to $900 per procedure with relatively low consumable costs while delivering substantial revenue per patient interaction.
High-margin specialty revenue streams include:
Cash-pay procedures are especially attractive because they eliminate the billing cycle. You charge, the patient pays, and the money hits your account the same day. No claim denials. No 30–60 day waits. No write-offs.
Revenue Driver #4 — Chronic Care Management (Recurring Monthly Revenue)
This is one of the most underutilized revenue streams in primary care and it’s remarkably powerful once implemented.
Chronic Care Management (CCM) is a Medicare and insurance-reimbursed program where clinics are paid monthly to manage patients with two or more chronic conditions (diabetes, hypertension, COPD, etc.) outside of traditional office visits.
Chronic care management alone can generate $700 to $1,000 annually per enrolled patient, providing a predictable recurring revenue stream.
If your clinic has 200 patients enrolled in a CCM program, that’s $140,000–$200,000 in additional annual revenue collected monthly, with relatively low labor costs. This is the closest thing to SaaS-style recurring revenue in a clinical setting.
Other recurring revenue models include:
- Remote Patient Monitoring (RPM): Medicare reimburses monthly for tracking chronic patients via connected devices (blood pressure monitors, glucose meters)
- Wellness memberships: Direct-pay monthly subscriptions for preventive care, same-day access, and health coaching
- Annual wellness visits: Billable preventive services for Medicare patients.
Revenue Driver #5 — Telehealth Services (Lower Cost, High Volume)
Telehealth expanded dramatically post-2020 and has cemented itself as a permanent revenue stream for forward-thinking clinics. The overhead per telehealth visit is significantly lower no exam room setup, faster throughput, and the ability to serve patients across a wider geographic area.
Telehealth works especially well for:
- Mental health follow-ups and therapy sessions
- Medication management visits
- Chronic disease check-ins
- Post-procedure consultations
A provider can see more patients per day via telehealth than in-person, improving revenue per hour without adding staff or space.
Revenue Driver #6 — Clinical Trials and Research Participation
This one is less common but can be highly lucrative for the right clinic. Pharmaceutical and biotech companies pay clinics to enroll eligible patients in clinical trials.
Clinical research is a way to add income streams to a practice, as well as contribute to science. By joining up with clinical research organizations or pharmaceutical companies conducting research, a practice can offer new clinical options to patients with certain conditions while adding to income diversity. The revenue from these clinical trials can be quite significant.
Clinics with a focused patient population (diabetics, oncology, cardiovascular) are especially attractive to trial sponsors. Beyond the financial benefit, trial participation often enhances the clinic’s reputation and attracts specialist patients.
Revenue Driver #7 — Cash-Pay and Direct-Pay Services
One of the fastest-growing revenue models in healthcare is the deliberate shift toward cash-pay services either as a complement to insurance-based revenue or as a standalone model (Direct Primary Care, or DPC).
Medical practices that offer cash-based services like cosmetic procedures, medical spa treatments, or weight-loss programs can generate additional income. Cash-based services may have a lower revenue per instance, but patients are likely to return repeatedly contributing more to overall profits in the long run.
Why clinics love cash-pay:
- Zero billing overhead (no insurance staff needed)
- Immediate payment collection
- Higher net collection rate (you collect 100%, not 65–75%)
- Pricing control — you set your own rates
DPC practices typically charge patients $50–$150/month in a subscription model, with unlimited primary care access. This model is growing rapidly among physicians who want predictable income without insurance administrative burden.
What Does a Clinic Actually Earn? Monthly Revenue Benchmarks
Medical clinics in 2025 typically generate between $30,000 and $50,000 monthly, with profitability heavily dependent on service mix, operational efficiency, and patient retention strategies.
That’s a wide range, and the gap is almost always explained by service mix. A clinic relying solely on low-margin primary care consultations will sit at the lower end. A clinic that layers in specialty procedures, CCM, telehealth, and cash-pay services can blow past that ceiling.
The formula is simple: Revenue = Patient Volume × Revenue Per Visit × Net Collection Rate
Each variable is a revenue lever. If you see 20 patients per day at $150 average revenue and a 70% collection rate, you generate $2,100 per day. If you optimize to 25 patients at $180 average (by adding ancillaries) and improve collection to 75%, that jumps to $3,375 per day — a 60% revenue increase from the same clinic with the same providers.
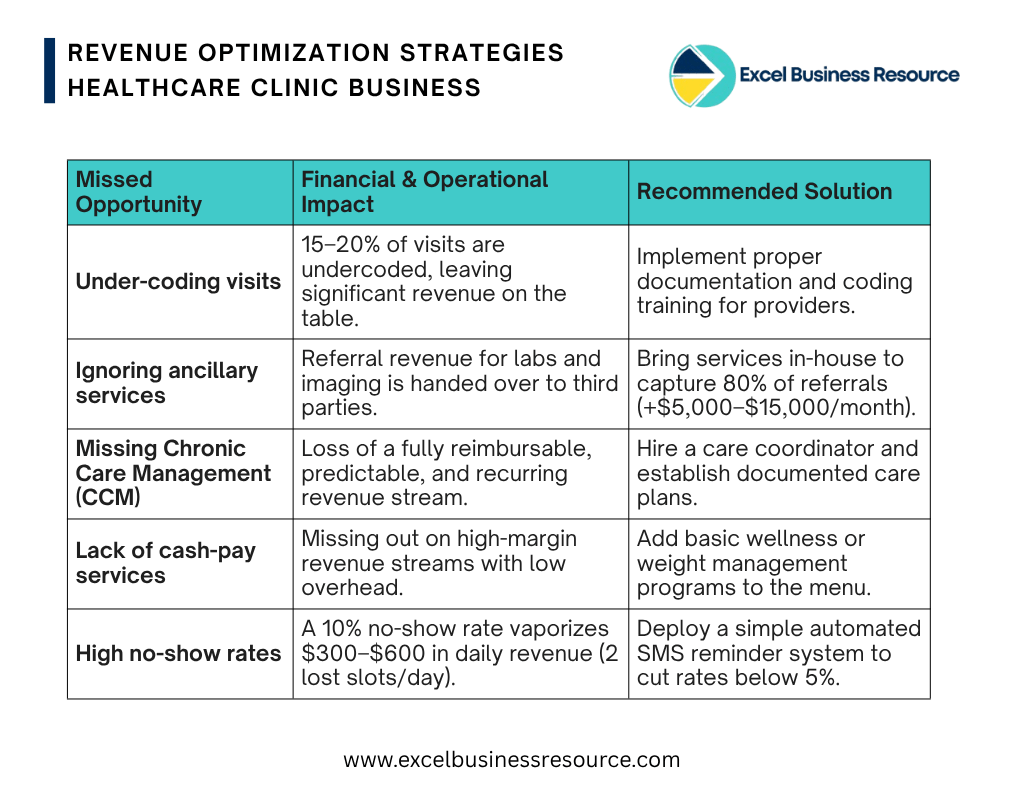
The Revenue Drivers Most Clinics Miss
Working with 100+ startups and healthcare businesses on financial modeling and FP&A at Excel Business Resource, we see the same missed opportunities repeatedly:
1. Under-coding visits — Providers habitually bill lower-complexity codes to avoid audits. Proper documentation training often reveals that 15–20% of visits are being undercoded, leaving real money on the table.
2. Ignoring ancillary services — Many clinics refer out for labs and imaging, handing revenue to third parties. An in-house lab that captures 80% of those referrals can add $5,000–$15,000 monthly.
3. Chronic Care Management not offered — CCM is a fully reimbursable, recurring revenue stream most primary care clinics never set up. It requires a care coordinator and a documented care plan — that’s it.
4. No cash-pay services in the menu — Even a basic wellness program or weight management service adds a high-margin cash stream without significant overhead.
5. High no-show rates eating capacity — A 10% no-show rate on 20 scheduled daily visits is 2 provider slots lost every day. That’s roughly $300–$600 in daily revenue vaporized. A simple SMS reminder system can cut this to under 5%.
Before You Open: Build Your Revenue Model First
Here’s the most important thing we tell every clinic founder: build your financial model before you spend a dollar on build-out or equipment.
You need to know:
- How many patients per day do you need to cover fixed costs?
- What’s your break-even by service mix?
- How does your revenue change if your payer mix shifts 10% toward Medicaid?
- What does your burn rate analysis look like in Month 6 when patient volume is still ramping?
These aren’t questions you answer with guesswork. They require a proper Medical Clinic Financial Model — one built specifically around the revenue drivers, cost structure, and KPIs of medical clinic business.
At Excel Business Resource, we’ve built one for you. Our investment-ready Medical Clinic Financial Model Excel Template includes:
- Revenue driver modeling by service line — consultations, diagnostics, specialty procedures, CCM, and telehealth
- Monthly financial projections for 5 years with built-in scenario analysis
- KPI dashboard tracking utilization rate, revenue per visit, net collection rate, and more
- Break-even analysis based on your actual patient volume and service mix
- Working capital forecasting and cash runway model
- Payer mix sensitivity analysis — see how your revenue changes if insurance vs. cash-pay ratios shift
- DCF Valuation output for investor presentations.
This is the exact type of financial model we build for our clients — available as a ready-to-use template so you can start planning today.
👉 Download the Medical Clinic Financial Model Template — Built for Founders & Investors
Final Thoughts
A medical clinic generates revenue through multiple overlapping streams — and the smartest operators treat each one as a distinct business within the business. Consultations provide volume. Diagnostics add margin to each encounter. Specialty procedures and cash-pay services unlock premium pricing. Chronic care management builds recurring revenue. Telehealth scales reach.
The clinics that build real financial success don’t rely on any single stream. They architect a service mix deliberately, model their unit economics carefully, track their KPIs monthly, and adjust based on what the data tells them.
Whether you’re a physician ready to go independent, an entrepreneur eyeing the healthcare sector, or an investor evaluating a clinic acquisition — your first step is the same: understand the revenue model completely before you commit.
Excel Business Resource has supported 100+ startups across FP&A, financial modeling, and business planning. Explore our full library of startup financial model templates including our healthcare business financial model designed specifically for clinic founders.
Founder's Asked Questions (FAQs)
Fee-for-service patient consultations remain the primary revenue driver, but clinics with the highest margins also generate income from ancillary services, specialty procedures, chronic care management programs, and cash-pay service lines.
Primary care clinics generate $100–$250 per visit at higher volume. Specialty clinics command $150–$900+ per visit at lower volume. Specialty clinics typically achieve higher per-patient revenue but require more upfront investment in equipment and credentialing.
Cash-pay aesthetic and regenerative procedures ($400–$900+ per treatment), in-house diagnostics, and chronic care management programs (recurring monthly revenue per enrolled patient) consistently deliver the best margins.
nsurance reimbursements create a lag between service delivery and payment. Clinics typically collect 60–75% of their gross charges after insurance adjustments and write-offs. Payer mix — the ratio of commercial insurance, Medicare, Medicaid, and cash-pay patients — is one of the most important revenue variables in any medical clinic financial forecasting model.
Start with your planned service mix, estimate average revenue per visit by service type, model patient volume growth month by month, and apply a realistic net collection rate. A financial projection model for medical clinic does this automatically and lets you test different scenarios before committing capital.